Forehead
Gender Differences:
There are 3 main differences between
masculine and feminine foreheads:
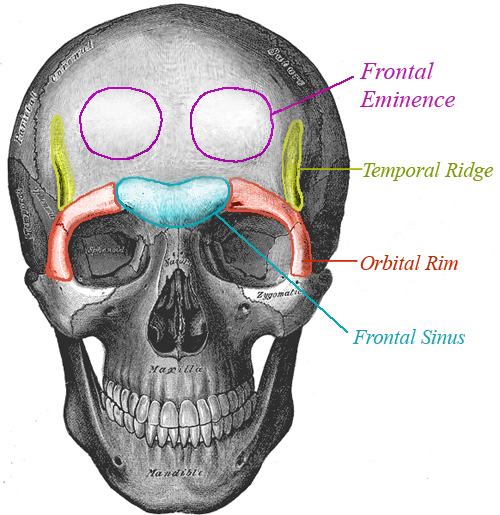
1. The most important difference between them is that masculine foreheads tend to have a ridge of bone running right across them at about eyebrow level called "brow bossing" (sometimes called "frontal bossing" or "the brow ridge") while feminine foreheads tend to be smoother and flatter and have little or no bossing. The bossing here has 2 parts to it - the "frontal sinus" which is in the middle, and the "orbital rims" which sit above the eyes (sometimes called the "supraorbital rims").
Brow bossing affects the expression of the face so a person with a masculine forehead usually looks harder or more angry, as opposed to the softer and more open expression that you tend to see with feminine foreheads.
2. The vertical ridges running up either side of the forehead (temporal ridges) and the rounded bumps on either side of mid forehead (frontal eminences) tend to be more pronounced in males.
3. Male foreheads often have a slightly backwards slope to them while female foreheads tend to be more vertical.
Here is a picture of a skull showing the key areas:
Surgical Options for Brow Bossing:
The orbital rim is usually solid bone and can simply be ground down. The surgeon can also open out your orbits to give you a more open, feminine expression. This is done by removing a little bone from the underside of the orbital rim and it has the additional effect of exposing more of your upper eyelids.
The temporal ridges and frontal eminences are solid bone too, and can be ground down in the same way as the orbital rims.
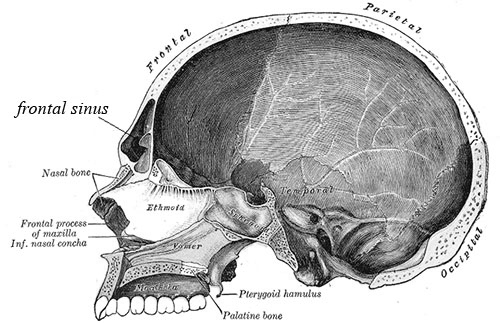
The middle third or so of the bossing is where you find the frontal sinus which is a hollow, air-filled cavity, and it is much more difficult to remove the bossing here. If the sinus has a thick wall of bone at the front, the bossing can, in theory, be removed by simply grinding down the bone, however in most people, the wall of bone is very thin, and that means it is not usually possible to grind the bossing away completely without breaking through it into the sinus. This would leave you with a hole in the forehead,
Here is a cross section through the skull so you can see the hollow frontal sinus clearly:
There is a debate about how the frontal sinus should be dealt with (more on that below in "The Great Forehead Debate" section) but first, here's a description of the 2 main approaches that surgeons take to this area:
1: Shave and Fill
Some surgeons grind down the wall of bone as
far as possible without breaking through into the frontal sinus, and then
build up the area around the remaining bossing with bone cement. The bone
cement smoothes out any visible step between the bossing and the rest of the forehead to give a smooth appearance.
2: Forehead Reconstruction
Other FFS surgeons perform a procedure called a "forehead reconstruction" where the wall of bone is removed and reshaped,
then the area around the sinus is ground down, before the wall of bone is fixed back in a new feminine position with titanium microplates and screws (older techniques use wires instead of plates and screws).
It's a bit like turning a 2 storey house into a 1 storey house by lifting off the roof, then removing the top floor before putting the roof back on.
Other Techniques:
Compression
Some FFS surgeons have used a compression technique in some cases in the past where the wall of bone is first weakened and then compressed into place. It then heals in the new position.
As far as I know, this is generally not done now.
Some Questions:
How thick is the frontal wall?
On average it ranges from 2 to 12mm as you can see from this scientific paper, but the inner surface undulates so it varies in thickness in different areas,
and according to this research by the FFS surgeon Dr Spiegel, the area 10 mm either side of the centre has an average thickness of only 2.6 to 2.9 mm. So there is typically very little that can be removed from that area by grinding alone.
How big are the plates and screws used in forehead reconstructions?
They are tiny - the plates are typically formed of two eyelets with a piece joining them together. They are about this size: O=O (if you are reading this text at about an average 12-point size) and usually one is placed either side to hold the wall in place as it heals. The screws are
also tiny, like spectacle screws - about the size of this: T
Can you feel the plates and screws through your skin?
No, they sit very flat against the skull, and the soft tissues sitting
over them are quite a lot thicker than most people realise.
Is it true that you can achieve exactly the same results with grinding as with reconstruction?
No, that is not only untrue, but in the vast majority of cases, it's a physical impossibility. See "The Great Forehead Debate" below for more on this.
How do you get to the forehead bones so you can operate on them?
To reach the bones of the forehead an incision can be made across the top of the scalp from ear to ear (this is called a
"coronal" incision). Putting the incision over the top of your head means that any scar will be well hidden by your hair, unless you are suffering from baldness. It is also possible to put the incision round the back of the head.
If you are having a scalp advance to lower your hairline at the same time as your forehead work then the incision will be made along the hairline instead of over the top of the head. Once the incision is made, the soft tissues of the forehead are then lifted out of the way to reveal the forehead bones.
Some surgeons access the forehead bones endoscopically using smaller incisions but with this technique it is only possible to do the "shave and fill" technique, and it cannot be used to perform a forehead reconstruction. Endoscopic forehead techniques are not more advanced than open techniques - most FFS surgeons can work endoscopically. The reason they don't, is that in most cases, the technique cannot achieve the best results in forehead feminisation.
What Happens to the Lining of the Sinus?
The frontal sinus has a lining of mucosal tissue. This can be left in place or it can be removed.
Facial Team and Dr Spiegel for example, retain it, while Dr di Maggio usually removes it.
Don't forehead reconstructions cause long-term sinus problems?
No. In fact, many surgeons report that people have fewer sinus problems after a forehead reconstruction. This is because when the sinus is opened, the surgeon can see if there are any problems in there and can then deal with them during the surgery.
It has been claimed by one surgeon that 30% of forehead reconstruction patients have on-going sinus problems. I have never seen any scientific evidence to support this despite extensive searches and requests to the surgeon. If you find the evidence, let me know. In the meantime, treat it as a completely unsubstantiated rumour. I have personally met a large number of post-op patients, as well as corresponding with many more and I have never come across the problem.
What about the slope of the forehead?
It is true that male foreheads tend to slope backwards more than female foreheads. You can't really correct this with surgery
without adding foreign material like bone cement which carries additional
complication risks. However, once the brow bossing is removed, the slope usually looks more vertical
because you have now set the lower part of the slope back a little. Also,
I do not think that the slope of the forehead is important in gender recognition. The key area is the bossing
- that's the bit that really makes people see masculine.
What about Frown Lines?
Reducing horizontal lines across the
forehead is rejuvenating, reducing vertical frown lines between the eyebrows is rejuvenating but also feminising because it softens your expression. The lines can be reduced with Botox, but for a permanent effect you can have the surgeon work on the underlying muscles during a brow lift or forehead feminisation surgery. Like Botox, this does reduce the lines but will also limit movement of the forehead muscles to some degree,
and one potential downside is that it is difficult to control the degree of
change symmetrically - this means that the muscles might be weaker on one
side than the other and that might add an asymmetry to your facial
expression. So I generally recommend Botox.
The Great Forehead Debate!
As I mentioned above, there is a great deal of heated debate in FFS circles from both patients and surgeons over whether option 1 (shave and fill) or option 2 (forehead reconstruction) is better in cases where the bossing is prominent but the frontal bone is thin.
Some feel that a reconstruction is too invasive and that disguising the bossing with the shave and fill technique is just as good as removing it; but others feel that disguising the bossing is an unacceptable compromise that can often leave the forehead with an unnatural bulge. They also feel that the shave and fill technique is too risky because it is difficult to control the degree of thinning of the bone.
The following pictures might help to explain the debate. Please bear in mind that the pictures are for illustration purposes only - they do not show all the details of forehead anatomy and they are not necessarily to scale. Let's start by looking at a forehead with strong bossing:

We can’t tell from looking at this picture whether the bone over the frontal sinus is thick or thin. To know that, we have to look inside, so lets look at 2 potential interiors for this forehead:

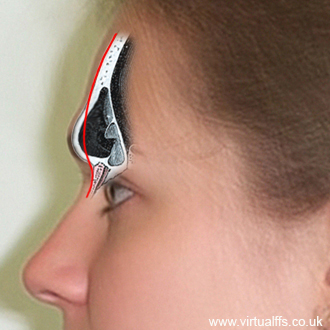
As you can see, they both have the same amount of bossing from the outside, but different bone thicknesses on the inside.
The first one (on the left) shows thick bone over the frontal sinus, the second one (on the right) shows thin bone. I have added a red line to show an ideal feminine bone structure. Most trans women have foreheads similar to the one on the right with the thin wall.
With the thick bone, the surgeon can grind it down to the ideal line and there will still be plenty of bone left to cover the frontal sinus as you can see from the amount of bone to the right of the red line.
With the thin bone you can’t grind it down to the ideal line or even very much at all without breaking through into the sinus. So in those cases (the majority) many FFS surgeons will perform a forehead reconstruction, taking the frontal wall off and placing it back in the new, feminine position as I described above.
After a forehead reconstruction, it ends up something like this:

So, grinding down thick bones, or doing a forehead reconstruction on thin bones both have the same result - the bossing is removed.
The controversy usually begins when a surgeon who does not, or cannot do forehead reconstructions, tries to tackle the thin-boned type of forehead with a shave and fill technique.
As I mentioned above, they approach it by grinding down what they can (sometimes just 1 or 2 mm) and then building up the areas around the bossing with bone cement to disguise it. Here's a picture to illustrate this approach (the bone cement is in yellow):

As you can see, although the new forehead is smooth, it bulges forwards of the red line.
Now, let's compare the end results for these 2 different approaches to the thin frontal bone problem. The picture on the left shows the result of the reconstruction technique and picture on the right shows the result of the shave and fill technique:


You can clearly see the bulge caused by the shave and fill technique. This is what I call a "dolphin forehead". I personally consider it an inferior and somewhat unnatural result, but some people don't mind it.
The flatter, reconstructed forehead on the left, is closer to the forehead the patient would have had if she had not gone through a male puberty, and that, in my opinion, is the goal of FFS. I call this concept "Puberty Reset".
In the case of medium-thickness bone, the difference in the end result between the reconstructed forehead and the non-reconstructed forehead is not as extreme as you can see in the next pictures:

As before, the picture on the left shows the reconstructed forehead and the picture on the right shows the shave and fill technique. However, although the difference is not as extreme, the result on the left is still, in my opinion, more natural and more feminine than the result on the right.
Some FFS surgeons like Dr Simon and Dr Capitán of Facial Team, do a reconstruction, even in cases where there is no frontal sinus at all. This is because the surface bone (called "cortical bone") is stronger than the more spongy bone beneath, so they prefer to set the strong bone back rather than grinding it away to expose the weaker, spongier bone.
Bear in mind that it is not possible to tell from the outside whether the bone is thick or thin or somewhere in between, and even a profile x-ray doesn't tell the whole story because, as I said above, the inner surface of the wall undulates so that the thicker areas hide the thinner areas when you are looking from the side. So looking at a profile x-ray profile of the sinus is a bit like looking across a mountain range from the top of a mountain - you can see how high the other mountains are, but you can't see how deep the valleys are.
A First Hand Account of Watching Forehead Reconstruction Surgery.
CONTENT WARNING: GRAPHIC SURGICAL DESCRIPTIONS!
The following account is based on watching the particular approach to forehead reconstructions taken by Dr Capitán and Dr Simon of Facial Team. Bear in mind that I may have misinterpreted some things and also that other surgeons will work in different ways.
The first thing the surgeons did was shave a thin strip of scalp and draw an incision line either side of the strip in pen (the strip is going to be removed so that when the incision is closed, the forehead will be lifted slightly).
They then inject lots of local anaesthetic into the incision site before making any cuts. This surprised me as the patient was, of course, unconscious. However, they explained that even though the patient is not aware of pain, the body itself still registers the pain and without the local anaesthetic, you start to see reactions like an increase in pulse rate. The local anaesthetic also helps to reduce bleeding.
The next surprise was just how thick the scalp is. When you feel your own,
you imagine it's quite a thin layer of skin, but it was at least a cm thick I would say.
Beneath these soft tissues is another layer called the periosteum. This is a thin translucent membrane that covers the bone, helping it heal and grow. This is peeled away very carefully with little prods that look a bit like spoon handles to expose the bone itself.
The next, interesting observation was just how much bone bleeds. I knew that bone is very much a living tissue, but I was surprised at just how much blood exudes from an exposed cranium. It makes the bone look surprisingly porous as the blood slowly seeps from fine holes. It's not an amount that causes problems, just more than I imagined.
The incision lines on the bone are marked in pencil. The surgeons told me that there is nothing better for marking bone than a pencil. The only problem is that pencils are made of wood, and that means they have to send them to a special lab to be sterilised.
Fine electric saws are used to cut around the frontal bossing and with a little tap, the frontal wall of the sinus is lifted off. The sinus itself is deeper than I expected and I can now confirm that despite a lot of misinformation on the internet, the frontal wall was, in both cases I observed, very thin. I would be surprised if either was more than 3 mm thick in the thinnest areas. The inside surface of the frontal wall undulates and you can see how a profile x-ray can only give a limited view when looking through an undulating plane.
The exposed edges of the sinus, the orbital rims and any masculine bumps
and ridges of the forehead were now ground down with electric burrs.
Personally, if I was the surgeon, this would be the most fun part!
The frontal wall was then trimmed and smoothed before being replaced using titanium microplates and screws. I had seen a lot of titanium microplates and screws in photographs, but was quite taken aback at just how tiny they are. It really is only a very small amount of titanium - probably somewhat less than many of us have in our jaws from normal dentistry. Once they are in place, the plates and screws are then shaved down flat with a burr, removing even more titanium.
The periosteum is now stitched back in place but two small gaps are left maybe 3 or 4 inches above the eyebrows. These are for the "endotines" - little triangular plastic devices about the size of fingernails with backwards-facing spines.
These help to hold the soft tissues of the forehead and the eyebrows in the right position as everything heals.
2 small, shallow holes are drilled into the skull in the appropriate
positions and the endotines clip in - it's very Ikea! They gradually dissolve over the next 6 months or so.
Now the soft tissues are lifted back into place. Emotionally, this was a difficult one to watch for me because watching the forehead work is quite abstract - you do not see the patients face, just an expanse of bone and a series of technical procedures performed with advanced tools. But when the soft tissues are lifted, there is the person, and scientific interest is suddenly replaced with compassion.
Finally, the scalp is stitched back together.
It was truly fascinating to watch forehead reconstruction surgery and I am very lucky to have had the chance. It certainly helps me in my own work visualising end results.